Anatomy and Physiology of Lactation
Learning Objectives
Knowledge and Understanding
- Understand the anatomy of human breasts and changes in breast structure and composition during pregnancy
- Understand hormonal changes regulating breast milk production and ejection (prolactin and oxytocin)
- Understand the stages of lactogenesis (I, II, and III) and factors affecting lactogenesis
- Management of common lactation problems
- Sore / cracked nipples
- Breast engorgement
- Mastitis
- Breast abscess
- Inverted / flat nipples
- Breast surgery
- Small / large nipples
- Not enough milk
- Other breast conditions
Anatomy of Human Breasts
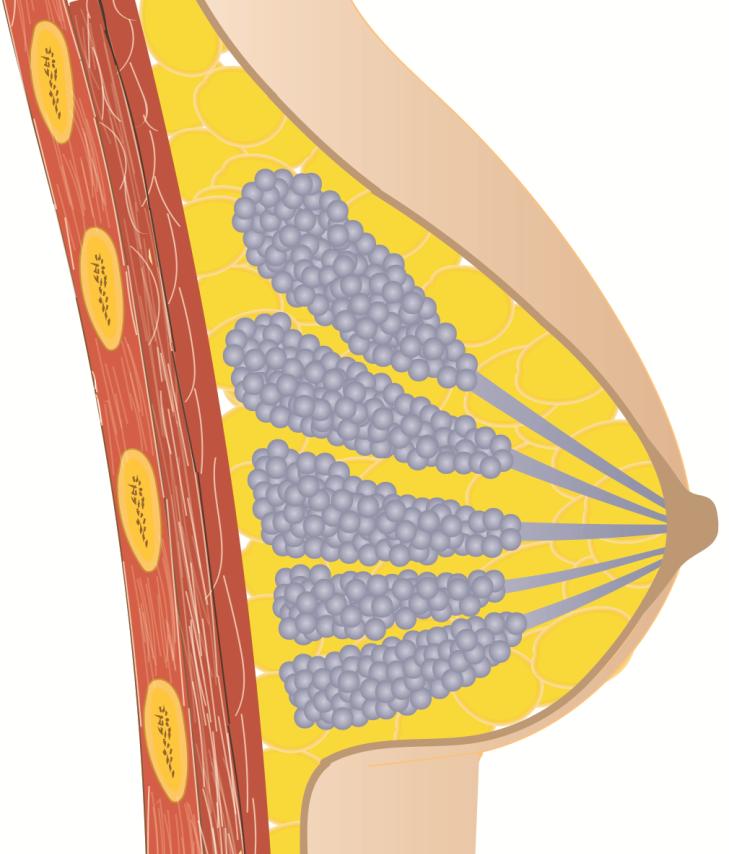
Breasts are made of numerous small sacs arranged in grape-like clusters called alveoli. Alveoli are very small cavities lined by cuboidal cells which produce and store milk. Many alveoli combine in groups to form a lobule. Each lobule is connected to a lactiferous duct which opens in the areola.
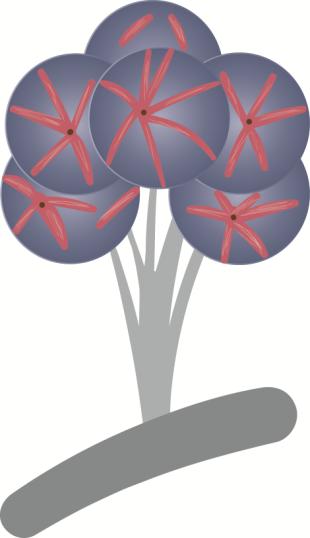
Alveoli are surrounded by myoepithelial cells which contracts with oxytocin stimulation causing milk ejection. This is called 'let down reflex'.
Lactiferous Ducts transports milk from alveoli to areola (dark skin around nipples).
Fat, muscles, and ligaments support the breast.
Changes in Breasts During Pregnancy
Development Before Pregnancy
Milk ducts and alveoli are not fully developed until pregnancy. Therefore, breasts do not have milk-producing capacity until pregnancy occurs.
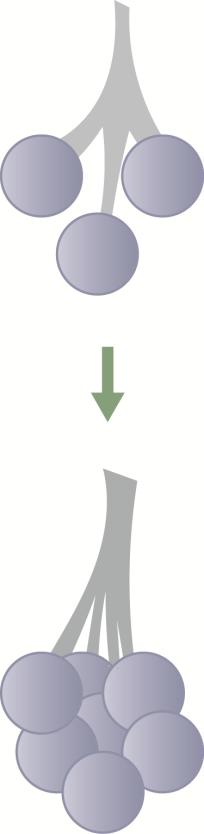
Lactogenesis I: Breast Development During Pregnancy
Pregnancy hormones cause rapid growth of milk ducts and alveoli.
Hormonal Effects:
- Estrogen and Growth Hormone: Increase the number of milk ducts
- Progesterone, Prolactin, and Placental Lactogen: Increase the number of alveoli
This process of rapid growth of the milk-producing mechanism during pregnancy is called Lactogenesis I.
Hormonal Changes During Pregnancy
Although breasts are capable of producing milk during pregnancy, circulating high levels of progesterone inhibit milk secretion. These high levels of progesterone are secreted from the placenta.
After Birth:
- Placenta is removed
- Rapid fall in circulating progesterone levels
- Leading to production of milk
Mothers having retained placental fragments have delayed milk production because these placental fragments continue to secrete progesterone which suppresses lactation.
Lactogenesis II:
- Mother secretes small amount of colostrum after birth
- Volume of milk rapidly increases after 36-48 hours
- This is called Lactogenesis II
Hormonal Regulation of Lactation
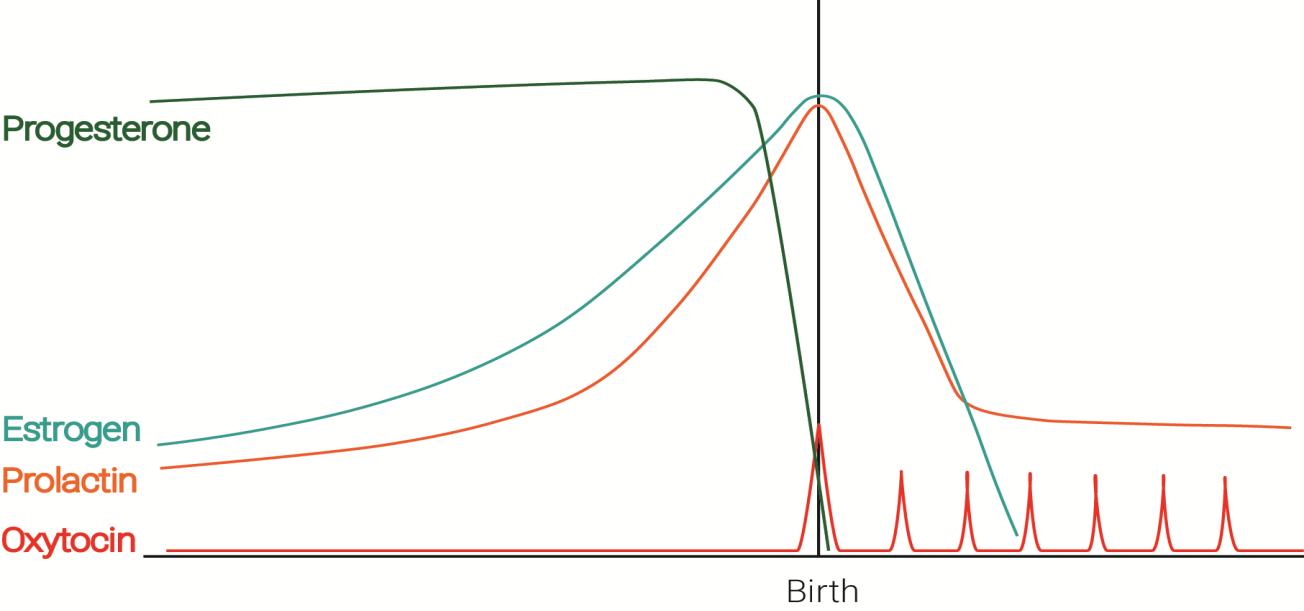
Key Hormonal Changes
Rapid fall in progesterone starts milk production after delivery
Steady prolactin levels maintain lactation
Breast stimulation by baby sucking causes oxytocin release leading to milk ejection from breasts
Two Essential Requirements for Milk Production
After development of breasts during pregnancy, two things are necessary:
- Prolactin Secretion
- Fall in Progesterone Levels
Prolactin: The Milk Production Hormone
Prolactin Function:
- Main hormone responsible for milk production
- Increases when the baby breastfeeds
- Early initiation of breastfeeding, frequent and exclusive breastfeeding boosts breast milk production by increasing prolactin levels
Prolactin Levels:
- Increased during breastfeeding
- Causes production of milk in alveoli
- Secreted from the anterior part of the pituitary gland
Pharmacological Support:
- Drugs which increase prolactin levels (such as domperidone and metoclopramide) can increase breast milk production
Oxytocin: The Milk Ejection Hormone
Oxytocin Function:
- Produced by the posterior part of the pituitary gland
- Released in response to suckling of breasts
- Causes 'let down' of milk
- Also causes contraction of the uterus, reducing postpartum bleeding
Oxytocin Stimulation:
- Produced in response to sensory stimulus to nipples
- Causes secretion of milk
Psychological and Emotional Factors

Positive Factors:
- Psychological and emotional response is required for successful breastfeeding
- Prolactin and oxytocin can be produced by:
- Close physical contact with the baby
- Smell and sound of the baby
- Back massage of mother reduces stress and increases oxytocin secretion. This technique is used for mothers presenting with problems of inadequate lactation

Negative Factors:
- Stress, anxiety
- Lack of sleep
- Separation of mother-baby
- May reduce milk production
Problems in Breastfeeding
1. Sore / Cracked Nipple / Nipple Trauma

Presentation:
- Burning pain during breastfeeding
- Redness and swelling of nipple and surrounding areas
- Fissures, blisters, or bruises over nipples
Causes:
- Vigorous rubbing during cleaning of nipples
- Use of soap for cleaning nipples
- Improper positioning of baby during breastfeeding
- Abrupt withdrawal of baby from breasts while still sucking
- Oral thrush in baby
- Improper use of manual suction-based breast pumps
- Syringes applied to inverted/flat nipples
Treatment:
-
Breastfeeding Technique:
- Start breastfeeding with the least affected breast
- Avoid pressure over sore areas
- Ensure proper attachment of baby during breastfeeding
-
Nipple Care:
- Nipples should NOT be rubbed during cleaning
- Do NOT use soap, detergent, or alcohol-based cleaners on nipples
- Keep nipples dry when not breastfeeding
-
Examination and Treatment:
- Examine baby for presence of oral thrush
- Treat baby's mouth and mother's breast for thrush
- Apply clotrimazole mouth paint if thrush is present
Nipple Shield for Treatment:

Application:
- Take a silicon nipple and enlarge its hole to the size of a pea
- Hold the nipple with index and middle finger against the painful areola over the breast nipple
- Let the baby suck at the silicon nipple
- With constant sucking, negative pressure develops which holds the nipple in place
- Holding fingers can now be removed
Benefits:
- Applying silicon nipple over sore nipple enables painless breastfeeding
- Promotes rapid healing of sore nipple
Use nipple shield only under supervision and guidance of a lactation counselor. Prolonged use may reduce mother's milk supply.
2. Engorgement of Breasts
Presentation:
- Increased size of breasts
- Feeling of tightness and heaviness in breasts
- With increasing engorgement, breasts become painful
- Diffuse reddish, swollen, and shiny areas over breasts
- Nipples become flat, preventing latching of baby

Causes:
- Inadequate emptying of breasts due to:
- Improper latching
- Delayed initiation of breastfeeding
- Nipple pain causing infrequent breastfeeding
- Ineffective sucking by the baby
Inverted nipple causing engorgement

Unilateral Engorgement:

Small nipple over one side causing breast engorgement because the baby could not latch on to this breast.
In case of unilateral breast engorgement, the cause is either the baby or the mother preferring one breast for feeding.
Prevention:
- Initiation of breastfeeding within first hour of birth
- On-demand breastfeeding at least 8-12 times a day
- Night-time breastfeeding at least 2-3 hourly
Treatment:
There is always an underlying cause of inadequate breast emptying. Treatment includes:
-
Identify and address the cause
-
Ensure complete emptying of both breasts:
- Proper attachment and positioning
- On-demand and exclusive breastfeeding
- Avoid top feeds
- Expression of breast milk by manual or electric breast pumps
-
Warm Compress and Massage:
- Apply warm compress over the affected breast
- Follow with gentle massage of breast in all four quadrants
- This helps viscous milk to be ejected out
-
Breastfeeding:
- Baby is now breastfed over the affected breast
- If baby unable to breastfeed, use electric or manual breast pump to empty the breast
-
Supportive Care:
- Paracetamol for pain relief and swelling
- Breasts should be supported with a wide bra
Note: There may be axillary nodular enlargement in some cases of engorgement which subsides on decompression of breasts.
3. Mastitis

Definition: Mastitis is the inflammation of breasts. It usually happens when engorgement of breast is not relieved.
Presentation:
- Affected breast is painful, red, and swollen
- Fever may also occur
- Breastfeeding is interrupted because of intense pain, further increasing breast engorgement
Causes - All Factors Causing Engorgement:
- Decreased frequency of breastfeeding
- Use of pacifiers or bottles for feeding
- Improper baby attachment
- Separation of mother and baby
- Abrupt weaning
Treatment:
-
Empty the Breasts:
- Exclusive breastfeeding
- Manual milk expression
- Breastfeeding should be continued
-
Comfort Measures:
- Provide warm compress for pain relief
- Give paracetamol for pain relief
- Mother should take plenty of fluids and bed rest
-
Antibiotics:
- Give antibiotics if fever and pain persist after 24 hours of treatment
-
Follow-up:
- If problem does not improve within 2 days, check for presence of breast abscess
Usual Sequence of Events:
Improper breast care or baby attachment -> Sore nipples
↓
Incomplete breast emptying (inverted nipples,
sore nipples, top feeding)
↓
Engorgement
↓
Mastitis
↓
Abscess
4. Breast Abscess

Definition: If mastitis remains untreated, it can cause abscess. Abscess is a collection of pus.
Presentation:
- Painful swollen lumps in breasts filled with pus
- Fever is present
Diagnosis:
- Ultrasound examination of breasts should be done to confirm findings
Treatment:
-
Surgical drainage of abscess along with complete course of antibiotics
-
Breastfeeding Management:
- Breastfeeding should be continued in breast abscess, if the abscess is NOT over nipple or areola
- It is safe and helps in treatment of the condition
- If necessary to withhold feeding in affected breast, it must be emptied regularly using breast pump
- Meanwhile, breastfeeding must be continued with the healthy breast
5. Inverted / Flat Nipples

Problem: Problems such as inverted nipple or small nipple can be effectively addressed even during the antenatal period.
Baby is unable to latch on inverted nipples, causing incomplete emptying of breast.
Inverted nipple can cause:
- Breast engorgement → Mastitis → Breast abscess
Antenatal Management:
- Nipple should be gently rolled between forefinger and thumb on regular basis
Use of Inverted Syringe:
- The use of an inverted syringe for application of suction is practiced at many centers
- Caution: This method should be used cautiously and gently, or it may cause nipple injury
Silicon Nipple Shield:

- Transiently, a silicon nipple shield can be used to facilitate latching
- The negative pressure generated by sucking of a newborn is far more gentle and appropriate for formation of the nipple
- Give direct breastfeeding without a nipple shield as soon as nipples are formed
Tube-Assisted Breastfeeding:

- Can also be used to initiate latching
- Or supplement the baby while maintaining baby's breastfeeding latch
Learn more: Inverted Nipples - Breastfeed India
6. Breast Surgery

Minor Breast Surgeries:
- Lumpectomy does not affect lactation
- Breastfeeding can normally be done in these cases
Major Surgeries:
- Surgeries which cause disruption of milk-producing and distribution mechanism
- Examples: breast implants
- Can affect lactation
7. Small / Large Nipples

Problem:
- Small or unusually large nipples may be difficult to latch on
- Incomplete emptying of breast can cause engorgement
Management:
- Examine the breasts
- Help the baby latch during initial few days
- Slowly the mother and baby will be comfortable with the attachment
8. Other Breast Conditions
Skin Diseases:
- In case of skin diseases of breasts like eczema, breastfeeding should be continued
Breast Size:
- Effective breastfeeding does NOT depend on size of breasts
- Every mother with any breast size can breastfeed
Blocked Duct (Pustule):

Mother having pustule (blocked duct) over left nipple causing:
- Inadequate breastfeeding from that breast
- Leading to breast engorgement → mastitis → breast abscess
Hand Expression Technique:
- Proper techniques of hand expression must be used
- Sliding of fingers during hand expression can cause breast abrasion

Positioning Issues:
- Sometimes there is no obvious problem with the breasts
- But mother still prefers to feed with one breast only because of some external problem with positioning (e.g., IV catheter in one hand causing pain)
- This may cause unilateral breast engorgement

9. Not Enough Milk
Normal Lactogenesis Process:
Day 1:
- Baby needs little amounts of milk on the first day
- Mother makes less than 100 mL of thick colostrum
- Colostrum is full of immunologic properties:
- Secretory immunoglobulin A
- Lactoferrin
Days 2-3:
- Volume of mother's milk rapidly increases
- This stage of copious milk secretion is called Lactogenesis II
Delayed Lactation:
- If it takes more than 72 hours to achieve Lactogenesis II, it is called delayed lactation
- Lactation counselors should immediately intervene rather than "wait and watch"
Common Causes of Delayed/Failed Lactogenesis:
- Delayed initiation of breastfeeding
- Maternal anxiety
- Giving pre-lacteal feeds
- Supplementing with top feeds
- Separation of mother with her baby
Never separate a mother from her newborn baby for unjustified causes. Separation of mother with baby decreases milk production.
Risk Factors for Failed Lactogenesis:
Maternal Factors:
- Diabetes
- Hypothyroidism
- Obesity
- Retained placenta
- Stress during labor and delivery
- Polycystic ovarian syndrome (PCOS)
- Sheehan syndrome
- Hypertension
- Breast surgery disrupting milk supply mechanism
- Cigarette smoking
Baby Unable to Suck Properly:
- Premature delivery
- Tongue tie
- Ineffective weak suck because of illness
- Pre-lacteal feeds given to baby
- Improper positioning and latch-on
- Use of pacifiers causing nipple confusion
Lack of early and frequent breastfeeding after birth is one of the most important risk factors for failed lactogenesis.
Therefore, a baby should be kept in skin-to-skin contact with her mother to ensure full stimulation of breasts and early breastfeeding.
Signs Baby is Receiving Inadequate Breastfeeding:
Baby will:
- Pass urine less than 6 times in 24 hours
- Be irritable/restless or not sleep well
- Lose more than 10% of birth weight
- Lose more than 5% of weight in 24 hours
How to Increase Milk Production
The best way to increase breast milk is to provide full stimulation to breasts and achieve the full milk-producing capacity of breasts.
Key Strategies:
-
Ensure Frequent and Exclusive Breastfeeding
- Breastfeeding should be on-demand
- Ensure at least 8-10 breastfeeding sessions per day
- Breastfeed at least 3-4 nighttime feedings
-
If Baby Cannot Breastfeed Directly:
- Due to prematurity or illness
- Mother should be supported to hand-express her breast milk
- A breast pump can also be used to help express breast milk
-
Early Initiation:
- Start breastfeeding as soon as possible after birth
- Skin-to-skin contact immediately after delivery
-
Avoid Interference:
- No pre-lacteal feeds
- No pacifiers or bottles
- No supplementation unless medically necessary
-
Support and Counseling:
- Reduce maternal stress and anxiety
- Ensure adequate rest and nutrition
- Provide emotional support and encouragement
Frequent breastfeeding and complete breast emptying are the most effective ways to establish and maintain adequate milk production.
References
-
Ramsay DT, Kent JC, Hartmann RA, Hartmann PE. Anatomy of the lactating human breast redefined with ultrasound imaging. J Anat. 2005 Jun;206(6):525-34. doi: 10.1111/j.1469-7580.2005.00417.x. PMID: 15960763; PMCID: PMC1571528. Available from: https://pubmed.ncbi.nlm.nih.gov/15960763/
-
Neville MC, Morton J, Umemura S. Lactogenesis. The transition from pregnancy to lactation. Pediatr Clin North Am. 2001 Feb;48(1):35-52. doi: 10.1016/s0031-3955(05)70284-4. PMID: 11236732. Available from: https://pubmed.ncbi.nlm.nih.gov/11236732/
-
World Health Organization. Infant and Young Child Feeding: Model Chapter for Textbooks for Medical Students and Allied Health Professionals. 2nd ed. Geneva: WHO; 2025. ISBN: 978-92-4-011373-2. Available from: https://www.who.int/publications/i/item/9789240113732
-
Berens P, Eglash A, Malloy M, Steube AM. ABM Clinical Protocol #26: Persistent Pain with Breastfeeding. Breastfeed Med. 2016 Mar;11(2):46-53. doi: 10.1089/bfm.2016.29002.pjb. Epub 2016 Feb 16. PMID: 26881962. Available from: https://pubmed.ncbi.nlm.nih.gov/26881962/
-
Amir LH; Academy of Breastfeeding Medicine Protocol Committee. ABM clinical protocol #4: Mastitis, revised March 2014. Breastfeed Med. 2014 Jun;9(5):239-43. doi: 10.1089/bfm.2014.9984. PMID: 24911394; PMCID: PMC4048576. Available from: https://pubmed.ncbi.nlm.nih.gov/24911394/
-
Dixon JM, Khan LR. Treatment of breast infection. BMJ. 2011 Feb 11;342:d396. doi: 10.1136/bmj.d396. PMID: 21317199. Available from: https://pubmed.ncbi.nlm.nih.gov/21317199/
-
Neifert MR. Prevention of breastfeeding tragedies. Pediatr Clin North Am. 2001 Apr;48(2):273-97. doi: 10.1016/s0031-3955(08)70026-9. PMID: 11339153. Available from: https://pubmed.ncbi.nlm.nih.gov/11339153/
-
Lawrence RA, Lawrence RM. Breastfeeding: A Guide for the Medical Profession. 9th ed. Philadelphia: Elsevier; 2021. ISBN: 978-0-323-68013-4.
-
Wambach K, Spencer B. Breastfeeding and Human Lactation. 6th ed. Burlington: Jones & Bartlett Learning; 2019. ISBN: 978-1-284-15156-5.