Preparation of Breastfeeding
Learning Objectives
Knowledge and Understanding
- Preparing the mother for breastfeeding during antenatal visits
- Hand hygiene
- Rooming-in after delivery
- Examination of breasts
- Hot fomentation and massage of breasts
- Hot fomentation of breasts
- Composition of Human Milk
Facilitators: Pediatrician, Lactation counselor
Facilitators will initiate each topic with a group discussion followed by a clinical demonstration and hands-on session. A breast mannequin will be used for demonstration of breast examination, massage of breast, hot fomentation and hand expression of milk.
This structured hands-on session will be followed by a clinical demonstration of counseling of mothers in the hospital.
Training resources: Running water supply, WHO hand washing chart, soap, disposable towels, breast mannequin
Preparing the Mother for Breastfeeding
Secretion of milk after birth depends upon the oxytocin-mediated let-down reflex which is stimulated when the baby suckles on the breasts. Therefore a baby must be breastfed as soon as possible within the first hour after birth.
Lactation counseling should start well before delivery and by the time the baby is delivered, the mother should know all the facts about breastfeeding.
What Should a Mother Know?
Use these points when counseling mothers during antenatal visits:
Early Breastfeeding:
- If the mother starts early breastfeeding, milk secretion will increase rapidly to meet the increasing demand of the baby
Nutritional Benefits:
- Breast milk provides all the essential nutrients specifically required by the baby
- Breastfeeding helps the baby to fight infection
Health Outcomes:
- Breastfed babies have a lower incidence of diarrhea and respiratory infections as compared to babies who are given top feed
Exclusivity is Key:
- Exclusivity of breastfeeding for the first 6 months is necessary:
- Immediately start breastfeeding the baby after birth
- Frequently breastfeed, especially during night
Avoid Supplements:
- Do not give supplements, formula feed, pre-lacteal feeds, ghutti, honey, water, etc. to the baby because these increase the risk of infection in newborn babies
Common Myths and Facts of Breastfeeding
Myth 1: Milk Secretion Starts Only After Third Day
Myth:
Milk secretion starts only after the third day, so the baby needs supplemental feeds until then.
Fact:
- Milk production starts late in pregnancy, even before delivery
- Breastfeeding immediately after birth and continued exclusive breastfeeding on-demand is important for milk ejection (oxytocin-mediated let-down reflex)
- Baby needs only small volumes of feed (5-15 mL per feed) during the first two days. Milk produced is sufficient to fulfill the baby's demands in most mothers
- Giving top feed risks infections in newborns. Do not give anything except breastfeeding unless advised by doctor
Myth 2: Mother's Milk is Too Less
Myth:
Mother's milk is too less for the baby, so additional supplement is required.
Fact:
- A newly born baby needs very little amount of milk, usually 5-15 mL per feed over the first two days
- The mother produces the required amount for her baby
- The baby's requirement increases over the second and third day after birth and by this time, the mother's milk increases in amount
Myth 3: Yellow Milk is Not Good
Myth:
Yellow milk is not good for the baby.
Fact:
- Yellow milk, also called colostrum, is rich in infection-fighting capability
- It is very essential for newborn babies because a newborn baby has very little immunity of their own
- Most of their immunity is derived from the mother
Additional Myths Associated with Cesarean Delivery
Myth 1: Mother Needs Rest, Baby Should Not Disturb
Myth:
Mother is weak after cesarean and needs a lot of sleep, so the baby should not disturb the mother and should not be kept near the mother.
Fact:
- The mother feels psychological satisfaction after breastfeeding. This increases her breast milk supply.
Myth 2: Milk Will Not Come Without Food
Myth:
Milk will not come because the mother is not taking food.
Fact:
- Short-term nutrition of the mother does not affect milk producing or secreting capacity after delivery
Myth 3: Baby Cannot Be Fed While Mother is Lying
Myth:
Baby cannot be fed because mother is lying straight on the bed.
Fact:
- Baby can be fed in prone position on first day and in side-position from second day onwards
- For effective breastfeeding, latching and attachment are necessary. The baby can attach in both these positions with some support.
Hand Hygiene
Lactation Counselors
Before Handling Mother or Baby:
- Lactation counselors must remove:
- Rings
- Bangles
- Sacred threads over wrists
- Wrist watches
- Wash their hands with soap and water following hand washing steps recommended by WHO
- Lactation counselors should trim hand nails appropriately
Mothers
Hand Hygiene for Mothers:
- Mothers should be guided to remove:
- Rings
- Bangles
- Sacred threads
- Wrist watches
- Wash their hands appropriately with soap and water
Care of the Breasts
Daily Breast Care
Routine Bathing:
- If the mother is taking routine bath, she does not require additional breast cleaning before breastfeeding
When Routine Bath is Interrupted:
- She can wash her breasts with water
- Mop them dry with cotton or a soft towel
Important Precautions
Nipple Care:
- Nipples should NOT be cleaned with detergent or soap as these can lead to cracked nipples
- Nipples should NEVER be rubbed for cleaning purpose
Rooming-In

Normal newborns should stay with their mothers in the same room, even during the hospital stay. This arrangement is called rooming-in.
The baby's crib should be placed near the mother's bed and the baby should be placed near the mother on the same bed when the mother is not sleeping.
Benefits of Rooming-In
For Breastfeeding:
- Enables frequent skin-to-skin contact of baby and mother
- Provides proper breast stimulation
- Ensures adequate breastfeeding
- Ensures proper lactation and adequate breastfeeding for the baby
For Baby:
- The baby stays warm and cries less
- Improved bonding between mother and her baby
Special Considerations
HIV Positive Mothers:
- Rooming-in should be provided in the same way as normal mothers
- If the mother has chosen not to breastfeed her baby, she can provide skin-to-skin contact without breastfeeding
Examination of Breasts
Systematic Approach to Breast Examination
Step 1: Observe Breastfeeding
- First, listen to the presenting complaints of the mother
- Watch the mother breastfeed her baby for at least four minutes
- Assess the problems regarding position, latching, and attachment
- Advise the mother about each stage of breastfeeding where shortcoming was detected using GALPAC approach
Step 2: Physical Examination When Problem Suspected
If a problem is suspected, e.g., engorgement, nipple problem, impending mastitis, then proceed with palpation of both breasts.
Palpation Technique:
- Palpation is done systematically in all the four quadrants
- Use clean flat surface of the fingers
- Palpation should be done in a gentle rotatory manner
- Aim to detect any swelling or lump
Step 3: Nipple Examination
- Check the nipple for:
- Cuts
- Fissures
- Sore nipple
- Cracked or inverted nipple
Step 4: Assess Milk Secretion
- Express the milk gently to see the milk secretion
- If the breasts are engorged, then express the milk either by hand expression or pump to relieve the pain and engorgement
Massage of Breast
Hot Fomentation Before Massage
Hot fomentation should be done before breast massage to soften the breast by increasing blood circulation and relieving pain.
Hot Fomentation Technique:
- A plastic bottle filled with warm water is applied subsequently to each quadrant of the breast
- Ensure that the water is not too hot or causing discomfort to the mother
- Bottle can also be wrapped in soft cloth
Breast Massage Technique
Massage Method:
- Massage is done by using flat surface of the fingers
- Fingers are gently moved in rotatory motion in all four quadrants
- Especially over the lumpy lobules which contain encysted milk (milk trapped in blocked ducts)
- Massage over these lumps dislodges the milk and allows it to flow through the ducts
Axillary Extension:
- Sometimes, swelling may extend up to the armpit
- This should also be gently massaged
Hand Expression of Breast Milk




Step-by-Step Hand Expression Technique
Step 1: Prepare
- Wash your hands with soap and water
- Gently massage the breasts with hands or soft cloth
- This will stimulate the oxytocin-mediated let-down reflex, making it easier to express milk
Step 2: Position Fingers
- Position your fingers and thumb on breasts outside the edge of the areola to make a 'C' shape
- Do NOT place the fingers or thumb over the areola
- Cup the breast with another hand for support
Step 3: Express Milk
- Gently squeeze forward while taking care that your thumb and fingers should not be over the areola
- Do NOT slide your fingers or thumb over the breasts
Step 4: Repeat and Rotate
- Release the pressure and repeat it while rotating your fingers and thumb to different positions of the breast
Step 5: Collect Milk
- Collect the milk in a sterile steel container
Step 6: Alternate Breasts
- Shift to the second breast once milk flow slows down in the first breast
- After expressing from the second breast, shift back to first
- Express from both breasts changing positions till milk flow completely stops
Composition of Human Milk
The composition of mother's milk changes according to the baby's needs. Mothers having preterm babies produce milk containing more protein, fat, lactose, and immune properties. This milk helps in the rapid weight gain of the baby and provides an extra boost to the immunity of the preterm baby.
Changes in Milk Composition Over Time
Colostrum (Just After Birth):
- The mother produces a little amount of thick yellow milk called colostrum
- Colostrum is rich in immunogenic components such as:
- Secretory immunoglobulin A
- Lactoferrin
- White blood cells
- Colostrum helps to develop the gut immunity of a newborn
Foremilk and Hindmilk
The composition of human milk also varies during feeding.
Foremilk (Beginning of Feed):
- The milk secreted in the beginning is called foremilk
- It contains more water which satisfies the thirst of the baby
Hindmilk (End of Feed):
- Gradually during feeding, the milk becomes thick
- The milk secreted near the end of feeding is called hindmilk
- It contains two to three times more fat as compared to foremilk
- It provides energy and helps in the weight gain of the baby
Although there is no actual switching point between foremilk and hindmilk and the transition is very gradual, the concept is important because it explains why the mother should always feed the baby from one breast till it is empty before switching on to the second breast.
Effect of Maternal Nutrition on Milk Production
General Principle:
- The milk production of mothers after delivery does not significantly depend on the nutritional status of the mother
- Although severe malnutrition leading to constant stress will suppress lactation, usually a mother who is underweight or has some degree of anemia can normally lactate
Nutrient Composition Variations:
- There is some difference in the nutrient composition of breast milk between mothers based upon their nutritional status
- Most of the milk is produced in cells lining the alveoli and it remains unaffected by maternal nutrition
- Vitamins and fatty acid content of milk are derived from the maternal stores and are affected if the mother is deficient
Conclusion:
- Therefore, maintaining a balanced diet for the lactating mother is important
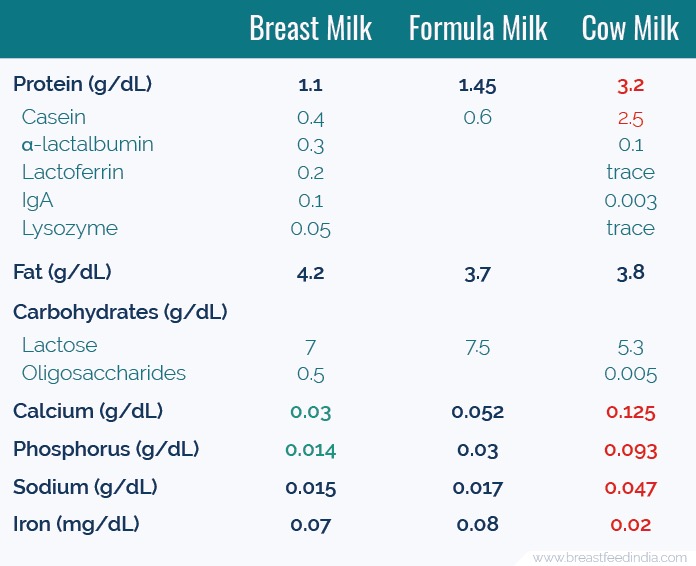
Macronutrients in Human Milk
Proteins
Protein Content:
- Milk of mother having a term baby is called term milk and its protein content is 1.1 g / dL
- This amount can go as high as 2.2 g / dL in milk of mothers having preterm babies
Protein Composition:
- Human milk contains whey protein which is considered as the most bioavailable protein on earth
- It also contains:
- Secretory immunoglobulin A
- Lactoferrin
- Lysozyme
- α-lactalbumin
- These proteins fight against bacteria and provide immunity
Fat
Fat Content:
- Human milk contains 4.2 g / dL of fat
Fat Composition:
- Fat present in human milk is rich in:
- Palmitic acid
- Oleic acid
- Long chain polyunsaturated fatty acids
Carbohydrates
Carbohydrate Content:
- Lactose is the main sugar present in human milk
- Oligosaccharides are also present in human milk which provides prebiotic properties to human milk
Micronutrients of Human Milk
Micronutrient composition of human milk vary according to the maternal diet and stores.
Vitamin Supplementation:
- Human milk has very low content of Vitamin K and Vitamin D
- Therefore:
- Vitamin K is injected to all newborns at birth
- Vitamin D is given to all infants up to one year of age
Bioactive Components of Human Milk
Human milk contains bioactive components. This means that it does not simply provide nutrition to a newborn, rather it affects multiple mechanisms of the body to improve the overall health of the baby.
Immune Components
Living Cells:
- Macrophages: Stimulate T-cell activity and helps in development of immune system of baby
- Stem cells: Helps in regeneration and repair
Proteins Provide Immunity:
- Secretory IgA, IgM and IgG: Direct immune protection
- Lactoferrin: Effective against bacteria, viruses and fungi
- Lactadherin: Helps in healing of intestine
Prebiotics:
- Oligosaccharides: Acting as prebiotics helps in development of probiotic microorganisms in gut which helps in digestion and prevents growth of harmful organisms
Anti-inflammatory Effects:
- Cytokines: Reduce inflammation
- TGF-β: Has anti-allergic effect
Growth Factors
Gut Maturity
- Epidermal growth factor: Helps in healing and maturation of gut
- Neuronal growth factor: Helps in development of enteral nervous system
Growth and Development
- Insulin like Growth factors (IGF): Helps in tissue growth
- Vascular endothelial growth factor (VEGF): Angiogenesis and tissue repair
Long-term Health Benefits
- Adiponectin: Reduced incidence of obesity later in life
- Erythropoietin: Prevention of anemia
- Calcitonin and somatostatin: Growth regulation
References
-
World Health Organization. WHO Guidelines on Hand Hygiene in Health Care. Geneva: WHO; 2009. Available from: https://www.who.int/publications/i/item/9789241597906
-
Ballard O, Morrow AL. Human milk composition: nutrients and bioactive factors. Pediatr Clin North Am. 2013 Feb;60(1):49-74. doi: 10.1016/j.pcl.2012.10.002. PMID: 23178060; PMCID: PMC3586783. Available from: https://pubmed.ncbi.nlm.nih.gov/23178060/
-
Andreas NJ, Kampmann B, Mehring Le-Doare K. Human breast milk: A review on its composition and bioactivity. Early Hum Dev. 2015 Nov;91(11):629-35. doi: 10.1016/j.earlhumdev.2015.08.013. Epub 2015 Sep 12. PMID: 26375355. Available from: https://pubmed.ncbi.nlm.nih.gov/26375355/
-
Gidrewicz DA, Fenton TR. A systematic review and meta-analysis of the nutrient content of preterm and term breast milk. BMC Pediatr. 2014 Aug 30;14:216. doi: 10.1186/1471-2431-14-216. PMID: 25174435; PMCID: PMC4236651. Available from: https://pubmed.ncbi.nlm.nih.gov/25174435/
-
Morton J, Hall JY, Wong RJ, Thairu L, Benitz WE, Rhine WD. Combining hand techniques with electric pumping increases milk production in mothers of preterm infants. J Perinatol. 2009 Nov;29(11):757-64. doi: 10.1038/jp.2009.87. Epub 2009 Jul 2. PMID: 19571815. Available from: https://pubmed.ncbi.nlm.nih.gov/19571815/
-
Jaafar SH, Ho JJ, Lee KS. Rooming-in for new mother and infant versus separate care for increasing the duration of breastfeeding. Cochrane Database Syst Rev. 2016 Aug 26;2016(8):CD006641. doi: 10.1002/14651858.CD006641.pub3. PMID: 27562563; PMCID: PMC9168801. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC9168801/
-
Lawrence RA, Lawrence RM. Breastfeeding: A Guide for the Medical Profession. 9th ed. Philadelphia: Elsevier; 2021. ISBN: 978-0-323-68013-4.
-
Wambach K, Spencer B. Breastfeeding and Human Lactation. 6th ed. Burlington: Jones & Bartlett Learning; 2019. ISBN: 978-1-284-15156-5.