Human Milk Banking
Learning Objectives
Knowledge and Understanding
- Lactation Management Center
- To understand the role of Human Milk Bank as a Lactation Management Centre
- Donors
- To identify and recruit donors, obtain medical history and laboratory investigations
- Education and support for mothers using CFD (Counseling, Breastfeeding, Donation of mother's milk)
- To understand and treat mothers presenting with lactation problems at Lactation Management Centres
- To use CFD approach - Counseling and solving lactation problems, Breastfeeding her own baby, and donation of only the extra milk
- Post-donation processing, storage, pooling, microbiological screening, distribution, and record keeping
- To understand the process flow of human milk banks
Facilitators: Pediatrician, Lactation counselor
This session will focus on the process of counseling by the means of CFD workflow.
Trainees shall understand the working environment of Human milk bank and perform hands-on at various stations in human milk bank.
Training resources: Human milk bank and associated counseling centre.
Human Milk Banking
Breastfeeding is the best method of feeding an infant. All mothers should be encouraged and supported to breastfeed their babies immediately after birth.
When Direct Breastfeeding is Not Possible
When the baby is sick or premature and is unable to breastfeed, mother's milk should be expressed and fed to the baby. Sometimes a mother's own milk is unavailable or insufficient. The next best option is pasteurized donor human milk.
"When it is not possible for the biological mother to breastfeed, the first alternative, if available, should be the use of human milk from other sources. Human milk banks should be made available in appropriate situations"
— WHO and UNICEF, 1980
Integration with Lactation Management

Human milk banks must be linked to maternal and pediatric hospitals and should implement breastfeeding support for mothers presenting with lactation problems, thereby functioning as lactation management centres.
Definition and Function
Human milk bank is an absolute non-profit organization which:
- Screens and recruits donors
- Collects donated human milk
- Processes donated human milk
- Stores donated human milk
- Distributes donated human milk to meet the needs of vulnerable newborns
Record Keeping:
- Human milk bank maintains the record of donors, recipients, donated and distributed milk
Donors
Donors are healthy mothers who are voluntarily willing to give extra breast milk to other babies after feeding their own baby.
Donors may also include mothers whose babies are hospitalized or mothers experiencing infant loss.
Screening:
- Donors are screened for HIV, Hepatitis B, Hepatitis C, and syphilis initially and every 6 months during the donation period
Who Can Donate?
✓ A mother who has fed her baby and is donating only the extra amount of milk
✓ A mother who needs to maintain milk supply while her baby has not been allowed to feed because of sickness
✓ A mother who understands the hygienic procedure to express milk manually or with help of a breast pump
Who Cannot Donate?
✗ A mother who is positive for HIV / Hepatitis B / Hepatitis C / Syphilis
✗ A mother who uses tobacco / smokes / is a drug addict or alcoholic
✗ A mother who is receiving chemotherapy / radiotherapy
✗ A mother seeking reward for her donation
Establishing and Maintaining Milk Supply
To establish good milk secretion (lactogenesis II), initiate breastfeeding immediately after birth.
If the baby cannot breastfeed because of sickness or prematurity, the mother should start expressing her milk as soon as possible (ideally within 6 hours). Support these mothers to express their milk using hand expression or breast pump.
A manual or electric breast pump can be used to express breast milk.
Why Electric Breast Pump is Preferable
Cycling Rate:
- Pumps with cycling rates lower than 25 cycles per minute are likely to be ineffective at expressing milk and can cause nipple and breast pain because they suction and pull for longer periods
- An ideal cycling rate should be 45 to 55 cycles per minute
Suction Strength:
- The suction strength of the breast pump should be adjustable between 0 mm Hg to 250 mm Hg (millimeters of mercury - pressure measurement)
- A pump with a vacuum above 250 mm Hg causes severe pain
Double Simultaneous Pumping:
- Double simultaneous pumps stimulate both breasts at the same time and increase the milk production of mothers
- This function is present in some electric pumps
Durability:
- Breast pumps to be utilized in Milk Banks and by lactation counselors should be durable
- Pumps made for home use are likely to have a short life span when used in Milk Banks
Hygienic Practices
Follow hygienic practices for collection of donor milk:
- Educate mothers about hand washing
- Educate mothers about milk expression
- Educate mothers about breastfeeding positions
Education and Support of Mothers Using C F D
What is CFD?
C = Counseling of mothers
F = Breastfeeding
D = Donation of mother's milk
CFD is an approach for mothers presenting with lactation problems at lactation management centres. In a hospital setting, lactation counselors can visit maternity wards and identify mothers having lactation problems.
Why CFD Approach?
Simplifies the Process:
- CFD approach simplifies the entire process of education of donors
- Helps in the establishment of milk supply in adequate quantities to ensure sufficient breastfeeding to their babies
- Motivates them to donate
Cultural Context:
- In contexts where mothers have limited formal education and face social constraints, any proposition they are unsure about may lead to refusal
- Wet nursing has historical precedent in many cultures
- The concept exists in historical narratives and is still practiced in some communities
Addressing Donor Concerns
Common Concerns and How to Address Them
Concern 1: "Are they asking my milk for their personal gains?"
- Solution: Explain to the mother how milk banking works and educate her about how she can save lives by donating
Concern 2: "What would the society say?"
- Solution: Tell her about historical examples as well as the prevailing practices of wet nursing
Concern 3: "What would I feed to my own baby if I sign the consent papers and give away all my milk?"
- Solution: Explain that breastfeeding her baby is the first and foremost priority. Only extra milk remaining after the baby is fully satisfied can be donated
Concern 4: "Other concerns"
- Solution: Resolve them all before receiving donation
Importance of Problem Resolution
Many mothers are likely to refuse when proposed to donate the milk because of concerns about the milk supply.
Prerequisites for Every Donation:
- Solving problems of lactation
- Education of mothers about hygiene
- Education about manual expression
- Establishing breastfeeding are necessary before every donation
Benefits of CFD Approach:
- In CFD approach, every mother undergoes resolution of her breastfeeding problem and initiates breastfeeding with the help of a lactation counselor
- This encourages mothers to understand the entire process and relieves the apprehension of the milk supply
Summary of C F D Approach
C = Counseling
- Lactation counselors should identify mothers facing lactation problems and resolve their issues by counseling and intervention
F = Breastfeeding
- Breastfeeding should be the mainstay of lactation counseling
- Establish breastfeeding in every baby leaving the Lactation Management Center
D = Donation
- If extra milk is left after breastfeeding, the mother can be motivated to donate it for newborns in need
Post-Donation Processing Workflow
The complete workflow for processing donated milk includes:
- Pooling
- Pre-pasteurization microbiological culture
- Pasteurization
- Post-pasteurization microbiological culture
- Storage of milk
- Transport
- Administration
Pooling
What is Pooling?
After the milk is collected from donors, it is pooled.
Milk from 3-5 donors is mixed together before pasteurization. This process is called pooling.
Purpose of Pooling
1. Sufficient Quantity:
- A mother's milk may not always be in sufficient amount to run a complete pasteurization process
- The quantity of milk to be processed is increased by pooling
2. Standardized Nutrient Composition:
- Every mother produces milk that is best suited for her baby
- The nutrient value of the milk produced by a mother differs according to the gestational age and postnatal age of her baby
- Pooling of milk ensures a homogenous nutrient composition of donor milk across batches
Pooling Process
Step 1: Thawing

- Donor milk is thawed (melted) in warm water bath before pooling
- Thawing is the controlled process of melting the frozen milk received when taken out from deep freezer
Step 2: Mixing

- Milk from 3-5 donor mothers is mixed under laminar air flow in a sterile container
Step 3: Preparing for Pasteurization

- After pooling, the milk is poured in sterile containers for pasteurization
Pre-Pasteurization Microbiological Culture
A sample from the pooled milk is sent for microbiological cultures.
Purpose of Culture
Culture determines the presence of bacteria in milk.
- Unpasteurized milk contains some bacteria despite best hygienic practices
Acceptance Criteria
General Bacterial Count:
- If the unpasteurized milk contains more than 10⁵ CFU/mL (Colony Forming Units per milliliter) of bacteria, it is discarded
Specific Harmful Bacteria:
- Some bacteria are more harmful than others because they produce heat-resistant toxins which can endure the process of pasteurization
- If the unpasteurized milk contains more than 10⁴ CFU/mL of Enterobacteriaceae or Staphylococcus aureus, it must be discarded
Quality Control Indicator
Presence of excess bacteria also indicates that the hygiene has not been maintained during the expression and collection process.
Action:
- Reinforce the hygiene and hand washing practices in Lactation Management Center
- Review the storage temperatures of donor milk
Pasteurization

Pasteurization is a process of specific heat treatment of milk.
Goals of Pasteurization
Pasteurization must meet two goals:
-
Sterilization of milk
-
Retention of immunological properties of human milk
Holder's Pasteurization Method

The time tested method for pasteurization of human milk which serves both these goals is Holder's process.
Process:
- Milk is heated to a temperature of 62.5 ºC for 30 minutes
- After this, the milk is rapidly cooled to 4ºC
Implementation:
- Process of Holder's pasteurization accomplished easily by automated pasteurizer
Critical Importance of Temperature Monitoring
Temperature monitoring is crucial to every pasteurization process.
Every degree rise in temperature above the recommended levels and every extra minute of heat causes undesirable damage to immunological properties of milk.
How Difficult Is It to Sterilize Milk?
No! It is not. It is done daily in homes. When milk is boiled at home, it gets clear of all the microbes. But that is all we want from dairy milk.
However, human milk is not the same as animal milk.
The Unique Challenge
Human milk is a bioactive fluid:
- It has immunological properties which protect babies from illness
- When the milk is heated, these immunological properties are destroyed
The Challenge:
- To clear the milk of microbes as well as to protect the immunological properties as much as we can, that is a challenge!
What is Retained After Holder Pasteurization?
After Holder Pasteurization, the following immunological components are retained (approximate values that vary by study):
- Approximately 70% of secretory immunoglobulin A
- 20% of lactoferrin
- 30% of lysozyme
Important Note:
- Milk loses some immunological properties during pasteurization
- But if the temperature is not monitored and maintained strictly, this loss is significantly greater
Post-Pasteurization Microbiological Culture
After pasteurization, a sample of milk is sent for microbiological culture.
Acceptance Standard
Pasteurization process kills all bacteria in milk.
Zero Tolerance:
- If bacterial growth is detected in the culture of milk after pasteurization, the entire milk batch should be discarded
Quality Assurance
Presence of bacteria in post-pasteurized milk sample also indicates that there is a problem somewhere in the process of pasteurization.
Action Required:
- Pasteurization process should be evaluated and rectified
Storage of Milk
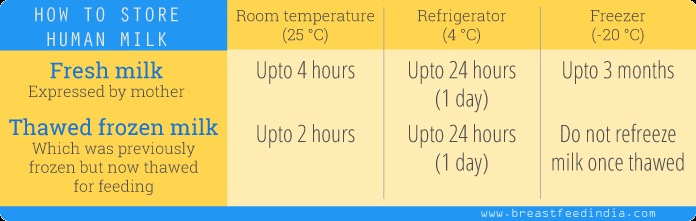
Short-Term Storage

Refrigerator:
- Donated milk is stored in simple refrigerator for less than 24 hours
Long-Term Storage

Deep Freezer:
- Deep Freezer at -20 °C is used to store milk for longer duration (up to 3 months)
- Depending upon the stage of processing, milk should be stored in pre-defined compartments of the deep freezer
- After pasteurization, milk is stored in the deep freezer
- All containers must be clearly labeled with donor ID, collection date, processing date, and expiration date
Transport

Transport Requirements
Heat Insulation:
- Human milk must be transported in heat insulating packs
- Protected by waterproof material
Cold Chain Maintenance:
- Cold chain must be maintained at all stages of transportation
Temperature Control:
- Frozen milk must be transported as such at a maximum temperature of 6°C
Administration
Thawing
When human milk is stored in a deep freezer, it becomes solid. Thawing is the process of liquefying it in a controlled way.
Thawing ensures a homogenous mixture of all the nutrients present in milk. Milk should be completely thawed and mixed before administering it to the baby.
Thawing Methods
When We Have Ample Time:
- Keep the milk in the refrigerator
- This way its temperature drops from -20°C to 4°C
- Use this milk within 24 hours
- Do not keep this milk at room temperature for more than 4 hours
When Short of Time:
- Prepare a warm water bath containing water at ~37°C
- Place the milk container in this water bath, ensuring that the water level does not touch the lid of the container, otherwise it may contaminate the milk
- When the milk is thawed but still chilled, it should be refrigerated
Important Warning:
- Thawed pasteurized milk should not be refrozen
- It increases hydrolysis of lipids and increases risk of contamination
Recipient Prioritization
Infants admitted in NICU having any of the following indications will be selected as recipients:
-
Premature and low birth weight infants
-
Infected newborns, especially with intestinal infections (necrotizing enterocolitis)
-
Infants not having access to their own mother's milk due to:
- Maternal death or serious illness
- Maternal HIV infection
- Maternal medications contraindicated with breastfeeding
- Inability of mother to produce milk despite support
-
Exceptional cases with medical justification
Administration of Donor Human Milk
Feeding Methods:
- Milk can be fed to the baby by either tube feeding or suthi/paladai feeding (traditional cup/spoon feeding method) as recommended by the treating doctor
Temperature for Preterm Babies:
- For preterm babies, milk should be warmed to 37°C
- This improves feed tolerance
Important:
- Do not give bottle feeding
Informed Consent
Consent from Recipients
Before administration of donor human milk, an informed consent must be signed by the parents of the baby.
The consent should include information about:
- Benefits and risks of donor human milk
- Alternative feeding options
- Pasteurization and safety procedures
- Donor anonymity and screening process
Consent from Donors
Consent should also be taken from mothers donating milk
The donor consent should cover:
- Voluntary nature of donation
- Screening requirements and testing
- How the milk will be processed and used
- Donor rights and confidentiality
References
-
World Health Organization & UNICEF. Joint Statement on Infant and Young Child Feeding. Geneva: WHO; 1980. Available from: https://www.who.int/news-room/fact-sheets/detail/infant-and-young-child-feeding
-
Ministry of Health and Family Welfare, Government of India. National Guidelines on Lactation Management Centres in Public Health Facilities. New Delhi: MoHFW; 2017. Available from: https://nhm.hp.gov.in/storage/app/media/uploaded-files/CLMC%20guidelines.pdf
-
PATH. Strengthening Human Milk Banking: A Global Implementation Framework. Bill & Melinda Gates Foundation; 2013. Available from: https://media.path.org/documents/MCHN_strengthen_hmb_frame_Jan2016.pdf
-
ESPGHAN Committee on Nutrition; Arslanoglu S, Corpeleijn W, Moro G, Braegger C, Campoy C, Colomb V, Decsi T, Domellöf M, Fewtrell M, Hojsak I, Mihatsch W, Mølgaard C, Shamir R, Turck D, van Goudoever J. Donor human milk for preterm infants: current evidence and research directions. J Pediatr Gastroenterol Nutr. 2013 Oct;57(4):535-42. doi: 10.1097/MPG.0b013e3182a3af0a. PMID: 24084373. Available from: https://pubmed.ncbi.nlm.nih.gov/24084373/
-
Peila C, Moro GE, Bertino E, Cavallarin L, Giribaldi M, Giuliani F, Cresi F, Coscia A. The Effect of Holder Pasteurization on Nutrients and Biologically-Active Components in Donor Human Milk: A Review. Nutrients. 2016 Aug 2;8(8):477. doi: 10.3390/nu8080477. PMID: 27490567; PMCID: PMC4997390. Available from: https://pubmed.ncbi.nlm.nih.gov/27490567/
-
Haiden N, Ziegler EE. Human Milk Banking. Ann Nutr Metab. 2016;69 Suppl 2:8-15. doi: 10.1159/000452821. Epub 2017 Jan 20. PMID: 28103607. Available from: https://pubmed.ncbi.nlm.nih.gov/28103607/
-
Infant and Young Child Feeding Chapter, Indian Academy of Pediatric; Bharadva K, Tiwari S, Mishra S, Mukhopadhyay K, Yadav B, Agarwal RK, Kumar V. Human milk banking guidelines. Indian Pediatr. 2014 Jun;51(6):469-74. doi: 10.1007/s13312-014-0424-x. PMID: 24986283. Available from: https://pubmed.ncbi.nlm.nih.gov/24986283/
-
Weaver G, Bertino E, Gebauer C, Grovslien A, Mileusnic-Milenovic R, Arslanoglu S, Barnett D, Boquien CY, Buffin R, Gaya A, Moro GE, Wesolowska A, Picaud JC. Recommendations for the Establishment and Operation of Human Milk Banks in Europe: A Consensus Statement From the European Milk Bank Association (EMBA). Front Pediatr. 2019 Mar 4;7:53. doi: 10.3389/fped.2019.00053. PMID: 30886837; PMCID: PMC6409313. Available from: https://pmc.ncbi.nlm.nih.gov/articles/PMC6409313/
-
National Neonatology Forum India. Evidence Based Clinical Practice Guidelines. NNF India; 2022. Available from: https://www.nnfi.org/nnf-cpg-guidelines.php