Breastfeeding
Quick Reference
The best milk for a neonate is breast milk. Breastfeeding provides:
- Optimum nutrition to neonate
- Easily available at appropriate temperature and easily digested
- Protects against infections, allergies, enhances emotional bonding between mother and baby.
- Breastfed babies have higher IQ and have less chances of developing hypertension, diabetes mellitus, coronary heart disease, appendicitis, liver disease and cancer in later life.
Breastfeeding her baby is also beneficial for mother:
- Reduces chances of postpartum hemorrhage
- Lowers the risk of breast and ovarian cancer in mother
- Decreases mother's workload involved in preparation of artificial feeds.
RECOMMENDED BREASTFEEDING POLICY
- Ensure exclusive breast-feeding during first 6 months of life.
- Start breast-feeding as soon as possible and within one hour of birth.
- Do not introduce ghutti, gripe water, honey or animal or powdered milk. They will reduce the breast milk intake by the baby. Give no artificial teats or pacifiers.
- Breast-feed day and night at least eight times or more on demand. Allow baby to feed at one breast till he releases the nipple on his own. Then offer him the other breast if the baby is still hungry, he will start suckling. However, if he does not feed from this breast now then offer this breast first at the next feeding session.
- Give complementary foods from 6 months of age.
- Continue breast-feeding up to 2 years of age or beyond.
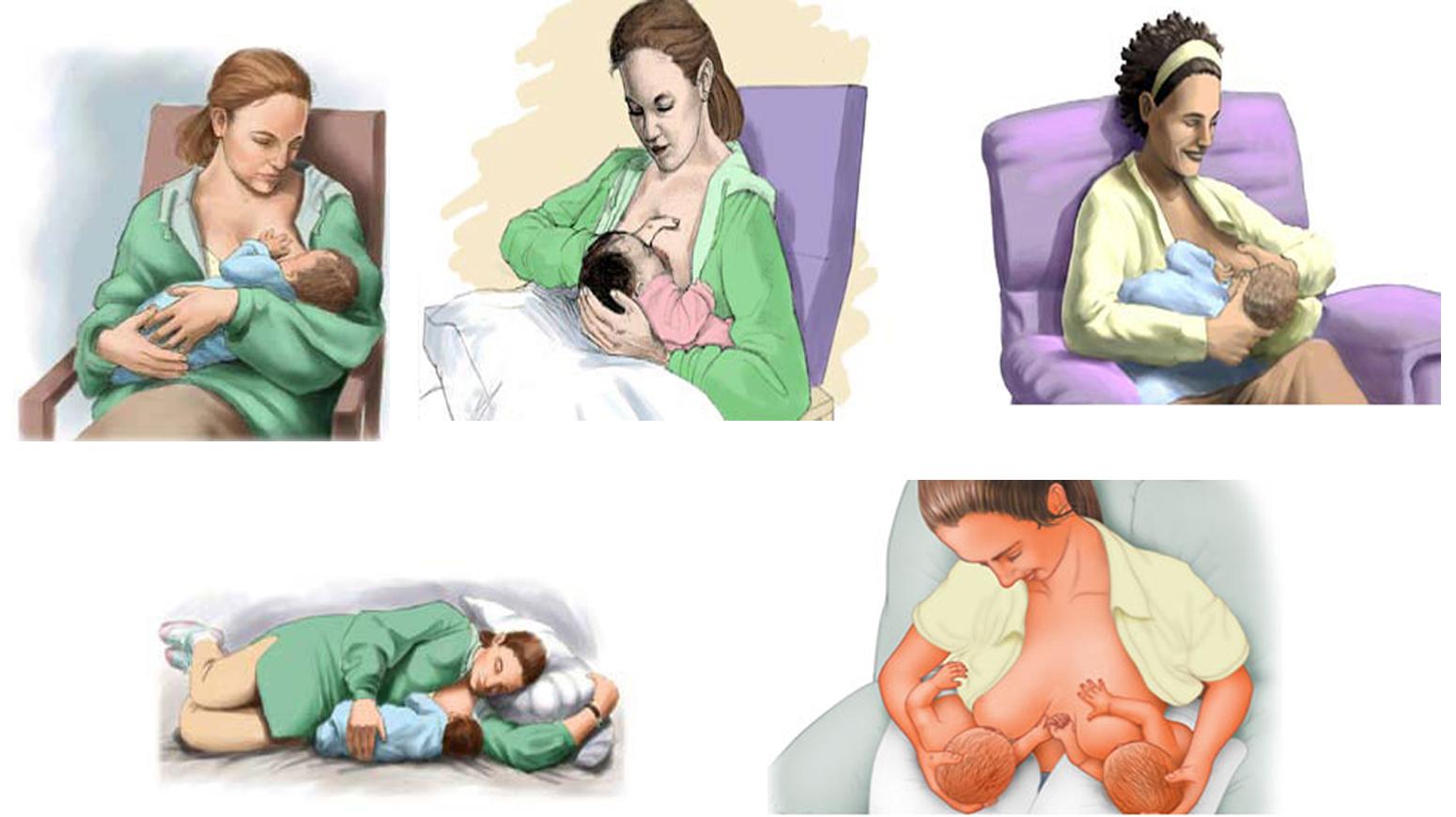
CORRECT POSITIONING DURING BREASTFEEDING
- Baby’s body is well supported.
- The head, neck and the body of the baby are kept in the same plane.
- Entire body of the baby faces the mother.
- Baby’s abdomen touches mother’s abdomen.
SIGNS OF GOOD ATTACHMENT OF BABY ON MOTHER'S BREAST
- Baby’s mouth is wide open
- Lower lip is turned outwards
- Baby’s chin touches mother’s breast
- Majority of areola is inside the baby’s mouth.
Breastfeeding Policy Document
This breastfeeding policy is based on recommendations by the Government of India, Indian Academy of Pediatrics (IAP), and National Neonatology Forum (NNF). It serves as a reference for healthcare institutions.
I. PURPOSE
To establish and promote a breastfeeding policy based on recommendations by the Government of India, Indian Academy of Pediatrics and National Neonatology Forum.
II. POLICY
A. Responsibility
This written policy will be regularly communicated to all health care staff who provide care for mothers and their newborns.
B. Staff Training for Policy Implementation
All nursing staff involved in care of mother-baby shall be responsible for acquainting themselves with the policy statement and acquiring the knowledge and skills to support the policy. Identifiable members of the professional staff of the hospital (doctors, nurses and lactation consultants) will assume primary responsibility for supervising this continuous educational process.
III. PROCESS
III-a. Process for Pregnant Mothers and Mothers with Healthy Newborns
A. Maternal Education
The obstetric and pediatric staff shall recommend exclusive breastfeeding for all babies in whom breastfeeding is not specifically contraindicated. Exclusive breastfeeding will be recommended as the ideal nutrition for newborns. The Hospital staff will not advise, provide or promote any breastmilk substitute to the mother and her baby. The Hospital will not provide formula marketing materials to mothers and will discourage promotional paraphernalia and marketing efforts in all areas accessible to patients.
Contraindications to breastfeeding include:
- Maternal HIV, human T-lymphotropic virus (HTLV)-1 and HTLV-2 infection
- Herpes simplex virus infection (when a lesion is present on the breast)
- Active tuberculosis (milk can be pumped and given to baby by another care provider)
- Mothers on medications that contraindicate breastfeeding (e.g., antimetabolites, therapeutic doses of radiopharmaceuticals, penicillamine)
- A newborn with galactosemia
When the breastfeeding is expected to resume after some time, the mother should be taught methods to maintain her milk production.
B. Initiation of Breastfeeding
Recommendations to promote successful breastfeeding will be followed:
-
Healthy term newborns with no evidence of respiratory compromise, will be placed and remain in direct skin-to-skin contact with their mothers immediately after delivery until the first feeding is accomplished, unless medically contraindicated.
-
Preterm babies (born before 37 weeks' gestation), babies having respiratory distress or cyanosis, major congenital anomalies that might lead to cardiorespiratory compromise, babies born through meconium-stained amniotic fluid and exhibit hypotonia or weak cry, babies born in the context of markedly elevated infection risk (maternal temperature ≥101°F), or have evidence of perinatal depression (e.g., decreased muscle tone, apnea, bradycardia) require immediate pediatric assessment instead of direct skin-to-skin contact with mother.
-
An alert, healthy newborn is capable of latching onto a breast without specific assistance within the first hour after birth.
-
Dry the baby, assign Apgar scores, provide identification bracelets to mother and baby, and perform initial physical assessment while the newborn is in direct skin-to-skin contact with the mother. The mother is an optimal heat source for the neonate.
-
Normal newborn care such as weighing, vitamin K prophylaxis should not delay early initiation of breastfeeding.
-
Newborns affected by maternal medication and primiparous mothers may require assistance for effective latch-on and initiation of breastfeeding.
-
Except under special circumstances, the newborn should remain with the mother throughout the recovery period.
C. Management of Lactation
Staff Assistance and Maternal Education
Nursing staff will assist each mother with breastfeeding within 6 hours of delivery. The mother should be guided so that she can help the newborn latch onto the breast properly.
During her hospital stay, mother shall be instructed and evaluated for:
Nutritional expectations:
- a) Expected feeding volumes in first 2 days (5–10 mL/feed in term newborn)
- b) Normal weight loss (average of 7%, not to exceed 10% in term newborns)
- c) Normal timing to regain birth weight (by day 10)
- d) Indicators of adequate hydration and nutrition (bright yellow stools by day 4–5)
Additional instruction on:
- Proper positioning of breastfeeding
- Hand expression of breast milk
Nursing staff taking care of mother-baby will evaluate the breastfeeding process for every baby daily, including observation of position, latch, and suckling. Each nursing shift will document these evaluations in the medical record.
Breastfeeding babies will be weighed each day. Weight loss of more than 7% in the first 72 hours indicates a possible breastfeeding problem and requires further evaluation of breastfeeding and correction of the problem.
Supplementation
Breastfeeding newborn does not need any supplementation; thus, routine supplements (water, ghutti, glucose water, formula, and other fluids) should not be given to breastfeeding newborns unless ordered by a doctor.
Rooming-In
The establishment of successful breastfeeding is facilitated by continuous rooming-in, both day and night. Therefore, the newborn will remain with the mother throughout the postpartum period, except under unusual circumstances.
Frequency of Feeds
Mothers should provide at least 8 feedings at the breast every 24 hours and on demand, i.e., whenever the newborn shows early signs of hunger, such as increased alertness, physical activity, mouthing, or rooting. Crying is a late sign of hunger.
Non-demanding babies should be aroused to feed if 4 hours have elapsed since last breastfeeding.
If the baby has not latched onto the breast or latches on but feeds poorly, the mother will initiate hand expression of breast milk. Any collected colostrum will be fed to the newborn by an alternative method. Skin-to-skin contact will be encouraged.
Use of Pacifiers
Pacifiers (also called dummies or soothers) should not be advised and use of pacifiers to breastfeeding infants should be discouraged.
Use of pacifiers interferes with breastfeeding by reinforcing maladaptive maternal breastfeeding practices and by disrupting suck mechanics. Pacifier use appears to be most strongly associated with termination of breastfeeding when it occurs in combination with improper newborn feeding or dysfunctional maternal styles of breastfeeding. Breastfeeding has been shown to have analgesic properties and also is an effective comfort strategy before or after a painful intervention.
D. Preparation for Discharge
All breastfeeding newborns will be assessed by a doctor for jaundice, adequate hydration, and age-appropriate elimination patterns. If a newborn is not latching on or feeding well by the time of discharge, the feeding plan will be reviewed and the baby should be followed-up within 24 to 72 hours of discharge.
III-b. Process for Mothers Who Deliver Prematurely or Are Separated From Their Newborns for Medical Reasons
A. Maternal Education
Mothers having premature or sick babies may be more concerned about the health-related issues of her baby rather than the benefits of human milk for their newborns. Doctors and nurses will therefore stress the protective properties of breast milk and recommend mothers to provide expressed breast milk for the baby.
B. Initiate Pumping
When direct breastfeeding is not possible, expressed breast milk is the preferred diet for sick or premature baby. Banked donor human milk may be a suitable feeding alternative for newborns whose mothers are unable to provide their own milk. Human milk banks adhere to strict quality control of screening and testing of donors and pasteurization of milk before distribution.
As soon as it is appropriate, the doctor should discuss human milk and its role in the preterm newborn's care, and the urgency to begin expressing or pumping. The responsibility for initiating and maintaining an expressing or pumping routine (at least 6 times/day with a hospital-grade breast pump) will belong to the nursing staff and should begin within the first 6 hours postpartum, or as soon after delivery as the mother is stable (not "recovered"). The aim is to mimic the optimal breastfeeding stimulation provided by a healthy full-term newborn.
C. Management of Lactation
Mothers who are separated from their newborns for more than 8 hours will be:
- Assisted with and instructed on how to hand-express colostrum
- Encouraged and taught how to provide small volumes of fresh colostrum for their newborn
- Encouraged to use only hospital grade breast pumps for expression of breast milk for their newborn
- Encouraged to practice skin-to-skin care as soon as the baby is stable
- Encouraged to initiate nonnutritive suckling as soon as mother's and baby's condition permits
- Encouraged to initiate breastfeeding on demand as soon as mother's and baby's condition permits
- Provided anticipatory guidance, when appropriate, on management of engorgement
References
- Indian Academy of Pediatrics. IAP Policy on Infant Feeding. Indian J. Pediatrics. 1995;32:155-164
- Indian Academy of Pediatrics, Infant and Young Child Feeding Chapter. Human Milk Banking Guidelines. Indian J. Pediatrics. 2014;51:469-474
- National Neonatology Forum. Evidence based Clinical practice Guidelines of Breastfeeding. www.nnfpublication.org. 2010
- Ministry of Human Resource Development. Department of Women and Child Development. National Guidelines on Infant and Young Child Feeding. http://wcd.nic.in/nationalguidelines.pdf
- World Health Organization. 10 Facts on Breastfeeding. www.who.int. July 2015
Document Information
Version: 1.0
Published: August 20, 2015
Contributors: Dr Chetan Meena, SMS Medical College, Jaipur